_haemorrhag.tiff)
_focal_necrosis__inam.tiff)
Note
Piscirickettsiosis is a significant infectious disease of farmed fish, first described affecting salmonid aquaculture in Chile with the earliest cases in the 1980s (Rozas and Enriquez 2014). The disease, also known as salmon rickettsial septicaemia (SRS), has subsequently been reported affecting salmonids in Australia, Ireland, Scotland, New Zealand, Norway and Canada (Brocklebank et al. 1992; Brosnahan et al. 2016; Corbeil, Hyatt, and Crane 2005; Grant et al. 1996; Olsen et al. 1997; Rodger and Drinan 1993). The disease has traditionally been associated with the marine Gammaproteobacteria Piscirickettsia salmonis, a Gram negative facultatively intracellular bacterium (Fryer et al. 1992; Schober et al. 2023). This pathogen has also been reported to cause disease in non- salmonid farmed fish including sea bass (Dicentrarchus labrax) (Comps, Raymond, and Plassiart 1996), white seabass (Atractoscion nobilis) (Chen et al. 2000) and lumpfish (Cyclopterus lumpus) (Marcos-López et al. 2017) with pathogen detections in other species also recorded (Schober et al. 2023). This note reports the recent increase in clinical cases and disease impacts with SRS in marine farmed Atlantic salmon (Salmo salar) in Ireland and Scotland.
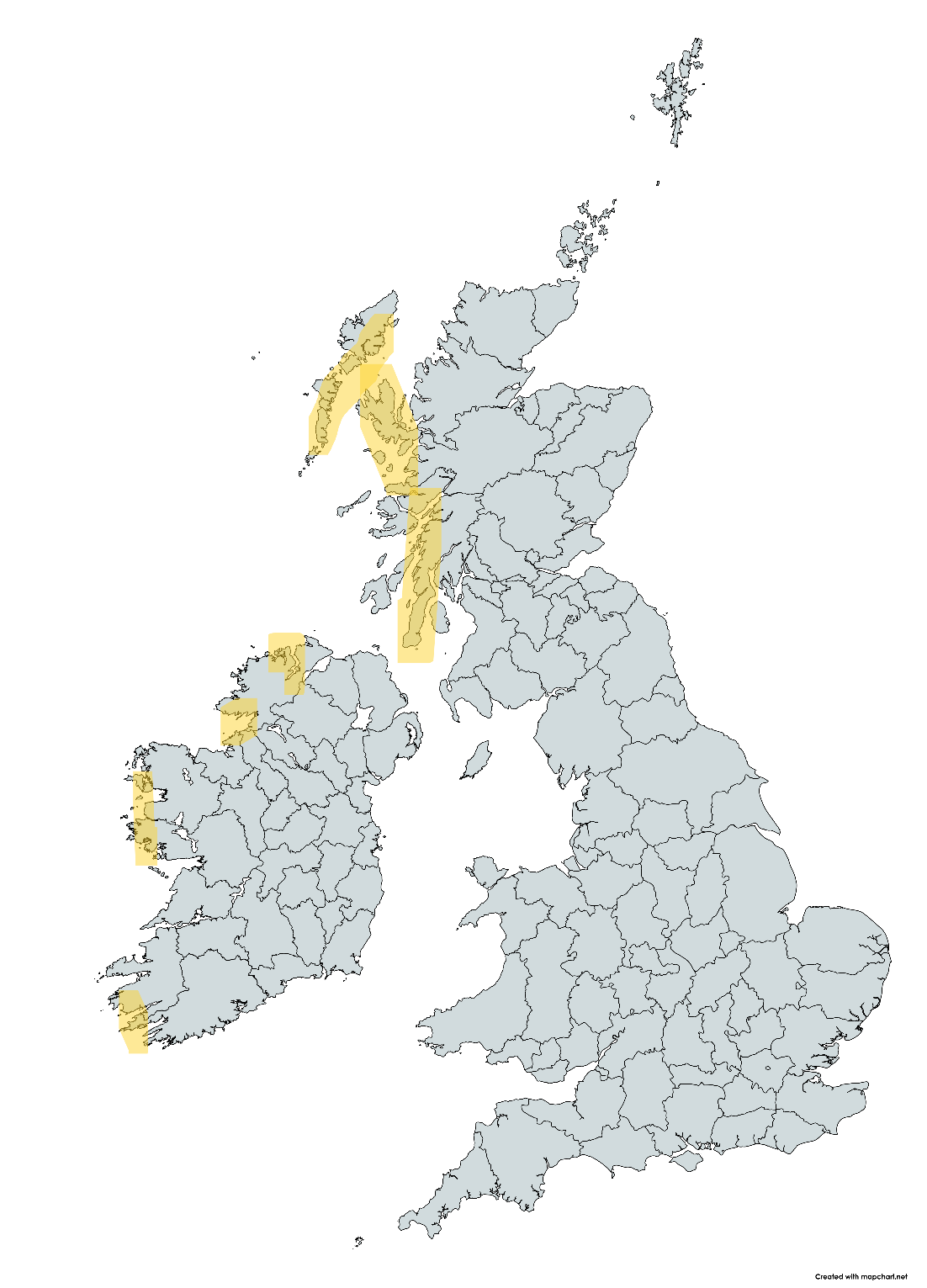
Despite SRS being confirmed in both Ireland and Scotland since the mid-1990s the number of clinical cases had remained low for over two decades with an estimated 0 to10 cases per annum between both countries (authors’ combined clinical experience). Mortality was of a low level in the majority of affected farms with minimal requirements for antibiotic treatments. However, since 2019 the clinical situation has changed and we have confirmed over 30 clinical SRS cases (defined as a distinct farm site population) per annum now confirmed between countries. SRS is also now responsible for the majority of prescribed antibiotic treatments in each country. The geographic areas affected include the North West, West and South West Ireland, mainland Scotland plus the inner and outer Hebrides, but not the Northern Isles (Orkney & Shetland) nor Northern Ireland (Fig. 1).
_where_piscirickettsiosis_has_caused_clinical_disea.png)
The clinical signs observed are consistent with those described previously (Grant et al. 1996; Rodger and Drinan 1993) and can include lethargy, anorexia, exophthalmia, skin colour change (increased melanisation), as well as skin lesions which initially may appear as haemorrhagic or pale patches, which can then ulcerate. Presentation of skin lesions can vary. Haemorrhagic lesions in the skeletal muscle, partly visible as skin blisters, and large ulcerative lesions on the peduncle are examples of less common presentations. External signs may not be present in all fish and, internally, gross pathological findings can include ascites, splenomegaly, cream-coloured patches on livers (which in some may be ring-shaped), pale swollen kidneys, mucoid contents in gastrointestinal tract as well as haemorrhages in visceral organs, on peritoneum, brain and in body muscle (Fig. 2). Gills can appear pale and haematocrits have confirmed a significant anaemia with packed red blood cell (PCV) levels of 2 to 20% in moribund fish (Branson and Nieto Diaz-Muno 1991).
_haemorrhag.tiff)
We have confirmed marine salmon can be affected by clinical piscirickettsiosis within 3 months after transfer to sea or at any stage up to harvest size. There is a distinct seasonal occurrence of clinical disease with the late summer-early autumn months showing peak mortalities coinciding with the periods of highest water temperature, however, clinical cases can also occur through winter months, although detections appear reduced below 12°C. Mortality may average 1 to 2% of all stock per week and cumulative losses, if untreated, can reach over 25%. Histopathology reveals a range of pathologies and cases may include multifocal ulcerative haemorrhagic, and often densely cellular, dermatitis and multifocal myositis, epi- and myocarditis, multifocal branchitis in gill filaments, random multifocal necrosis and inflammation in liver, spleen and kidney, as well as meningitis and ocular retrobulbar inflammation (Fig. 3). Basophilic intracellular microorganisms, with occasional cytoplasmic vacuolation, may also be observed in many organs as well as in leucocytes on blood smears (Fig. 3). Additional observations by the authors in Scotland and Ireland indicate that many, although not all, of the cases appear within two to four weeks of exposure to harmful algae, harmful gelatinous zooplankton, or following a non-medicinal bath treatment. It is also notable that SRS cases are often reported alongside gill pathologies such as complex gill disease (CGD) or amoebic gill disease (AGD). We have also regularly observed that outbreaks occur within three weeks of freshwater bath treatments for AGD in Ireland. This is consistent with observations in Chile (Rozas and Enriquez 2014) and with the recent emergence of bacterial diseases in marine sites in Norway (Stige, Colquhoun, and Oliverira 2025). A previous study has highlighted the detection of Piscirickettsia salmonis-like DNA in bacterioplankton DNA extracted from seawater in the Pacific (Mauel and Fryer 2001). It is considered likely that any cell damage associated with harmful plankton or bath treatments will facilitate the entry of P. salmonis into the fish, as the main routes of entry have been shown to be skin and gills (Smith et al. 1999). The above observations highlight the increased risk of SRS in previously unaffected geographic regions through the impacts from climate change, with the increased frequency of marine heatwaves and rising seawater temperatures of particular concern (Bravo et al. 2020; Rowley et al. 2024). Sea lice infestations with Caligus rogercresseyi have been significantly associated with piscirickettsiosis in Chile (Arriagada et al. 2019), and although in Scotland the sea lice species (Lepeophtheirus salmonis and Caligus elongatus) continue to challenge the industry, in Ireland the authors have not observed any association with piscirickettsiosis as the salmon lice burden of total mobile stages has been the lowest in 2023 and 2024 since records began in 1991 (D’Arcy et al. 2025).
_focal_necrosis__inam.tiff)
The aetiological agent, P. salmonis, has previously shown clonal diversity in samples from Ireland and Scotland (Reid, Griffen, and Birkbeck 2004). However, more recently a distinct Piscirickettsia species, provisionally named Piscirickettsia nova, has also been isolated on selective media from farmed Atlantic salmon clinically exhibiting SRS signs and histopathology, in both countries, and in the absence of P. salmonis (Teigene et al. 2025). Retrospective analyses of PCR kidney samples which had previously indicated detections of P. salmonis in Scotland from 2021 to 2024 have shown that over 50% of these (n = 28 to date) are P. nova (PatoGen laboratory data 2021 to 2024). The authors can confirm that this distinct Piscirickettsia species has also been detected by qPCR in the siphonophore Apolemia uvaria captured in southwest Ireland in August 2024. This siphonophore has caused significant challenges for farmed salmon in the North-East Atlantic (Madaro et al. 2025). There are no commercial fully authorised vaccines available in either country for piscirickettsiosis, however, autogenous vaccine use commenced in some sites in Ireland in 2024. In the absence of vaccine protection, antibiotic use has revolved around oral florfenicol or oxytetracycline and these treatments have shown apparent efficacy in mortality reduction in the majority of cases. Genetic or genomic selection for tolerance has been demonstrated in Atlantic salmon for P. salmonis (Correa et al. 2015; Moraleda et al. 2021) and highlights future methods to mitigate the impacts of the disease. In addition, improved biosecurity, especially with the risks associated with work vessel movements between regions and countries, will be vital to reduce the risk of spread of the disease. In Chile the benefits of site fallowing have been highlighted (Price et al. 2017). The cluster of SRS cases and P. salmonis detections in Norway in 2024 have also been a cause for concern (Holm et al. 2025).
There remain significant gaps in our knowledge with regard to this disease and, to clarify future research efforts, funding and knowledge exchange between countries, the SRS Initiative has been established. Details of the inaugural meeting held in Galway, Ireland are available here: www.srsinitiative.org